"
"
Team:Evry/Modeltr2
From 2013.igem.org










Final flush treatment model
Introduction
This model comes right after the Disease model. We now want to model the flush treatment by simulating a flush of iron-chelating bacteria.
Observations
Once our genetically modified bacteria are released in the duodenum, they produce siderophores to chelate the solved iron, thus making it unavailable for intestinal absorption. Then, they eventually flush out of the duodenum. The main hypothesis in this model is that the bacteria don't colonize the duodenum : they only flow through.
The goal of this model is to measure how efficient could this form of treatment be. Because too much parameters remain unknown, it is a theoretical simulation which will not give any numerical results.
Goals
This model was made to check if our first strategy was viable. It aims to answer the following question:
"Is it possible to chelate a significant amount of iron with a flush strategy?"
Assumptions
The same assumptions as in the previous model apply:- Our bacteria don't settle in the duodenum
- No regulation in the patient's iron absorption
- Constant iron flow
- Homogeneous fluid
- The bacterial quantity is constant
- The bacterial natural absorption is insignificant compared to the chelation
- The patient ingests 20mg of iron per day (Guideline Daily Amounts)
Materials and methods
 A : Total quantity of iron absorbed by the duodenum (mol)
A : Total quantity of iron absorbed by the duodenum (mol)
S : Quantity of solubilized iron (mol)
P : Total quantity of enterobactin produced by our population of bacteria (mol)
Q : Total quantity of chelated iron (mol)
N : Number of bacteria

The graph on the right explains the reasoning: for instance, the arrow with a + between N and P means that the variation of P has a positive linear term in N.
Where is our logistic function (which we will here abusively call activator).
is our logistic function (which we will here abusively call activator).Results
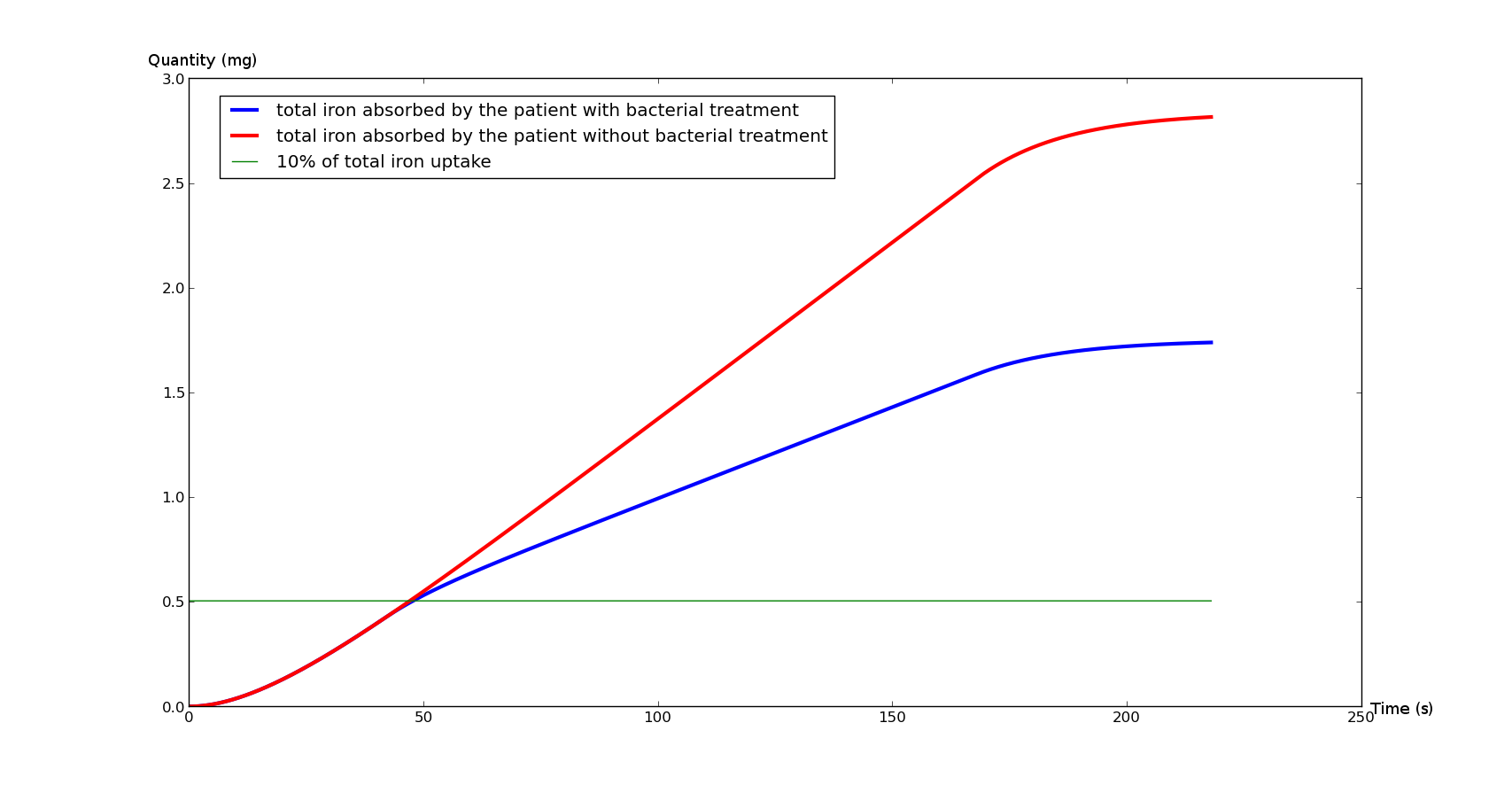
Figure 1 represent the iron absorbed by the duodenum during a meal. We can see the reduction of iron absorption in the duodenum

Figure 2 represent iron disolved in the chyme. This graph point out the influence of bacteria on the middle. The blue curve decrease significantly under the bacteria flux. That underline the fact that the treatment don't affect the absorption directly. After 150 secondes, chyme is no longer in the duodenum, thus the iron absorption is reduce in both cases.Baptiste: En fait je suis pas sûr que ça soit exactement ça, mais faudrait l'expliquer en tout cas même si c'est un artefact.
Parameters:
The simulations was made with following parameters:
| Name | Value | Unit | Description | Reference |
|---|---|---|---|---|
| Sp | 4.5*10^-9 | mol.s-1 | Iron pulse | [1][2] |
| v | 0.007 | m.s-1 | Chyme's flow average speed | [2] |
| L | 0.3 | m | Duodenum length | [3] |
| α | 0.03 | s-1 | Duodenum absorption rate | Disease model |
| δ | 2.65*10^-8 | mol-1 | Dimensional parameter | calculated |
| K | 100 | mol/s | Activator Magnitude | set |
| p | 0.005 | mol.s-1 | Value at zero of the activator | set |
| h | 10^-5 | - | Activator efficiency | set |
| d | 10^-9 | mol | Activator threshold | [4] |
There is a slight difference between the two cases, which would possibly allow us to fit the treatment to the patient's characteristics.
Conclusion
It is possible to significantly reduce intestinal iron intake if the patient takes one pill before or during each meal. This means that the patient would endure a lighter treatment : less bloodletting for people suffering from hemochromatosis, and less iron chelator's side effects for the thalassemia.
Models and scripts
References:
- Physiol Rev 93: 1721–1741, 2013 doi:10.1152/physrev.00008.2013 - Tomas Ganz "SYSTEMIC IRON HOMEOSTASIS"
- Calculated from : Computational Modeling and Simulation of the Human Duodenum - B. Hari, S. Bakalis, P. Fryer - 2012
- Wikipedia
- Calculated from : http://onlinelibrary.wiley.com/doi/10.1016/S0168-6445%2803%2900055-X/pdf p.217